Mar 17, 2021
CHWs At Work: Making a Difference for Oklahoma's Marshallese Community
 In 2014, a
statewide effort to disseminate primary healthcare
delivery innovations led to the creation of the
Oklahoma Primary Healthcare Extension System (OPHES).
This system, modeled after agriculture extension offices,
furthered its work by using County Health Improvement
Organizations (CHIOs). Allison Seigars, a member of one
of those CHIOs, remembers attending an early meeting with
another colleague and first hearing about Community Health
Workers (CHWs), their skill sets, and the value they
could bring to community healthcare outreach.
In 2014, a
statewide effort to disseminate primary healthcare
delivery innovations led to the creation of the
Oklahoma Primary Healthcare Extension System (OPHES).
This system, modeled after agriculture extension offices,
furthered its work by using County Health Improvement
Organizations (CHIOs). Allison Seigars, a member of one
of those CHIOs, remembers attending an early meeting with
another colleague and first hearing about Community Health
Workers (CHWs), their skill sets, and the value they
could bring to community healthcare outreach.
“We thought, wow! Would these professionals be the answer to working with our Marshallese population?” she said, sharing that multiple efforts to engage this local community from the Marshall Islands had met with little success.
Seigars is now the executive director of Rural Health Projects, Inc./Northwest Area Health Education Center (RHP/NwAHEC) located in Enid, Oklahoma. With her organization acting as the fiscal agent, a 2017-2020 Rural Health Network Development (RHND) Grant Program award allowed the Tri-County Health Improvement Organization (Tri-CHIO) to provide intentional outreach to the area's Hispanic and Marshallese communities. The RHND Program is administered by the Federal Office of Rural Health Policy (FORHP) within the Health Resources and Services Administration (HRSA).
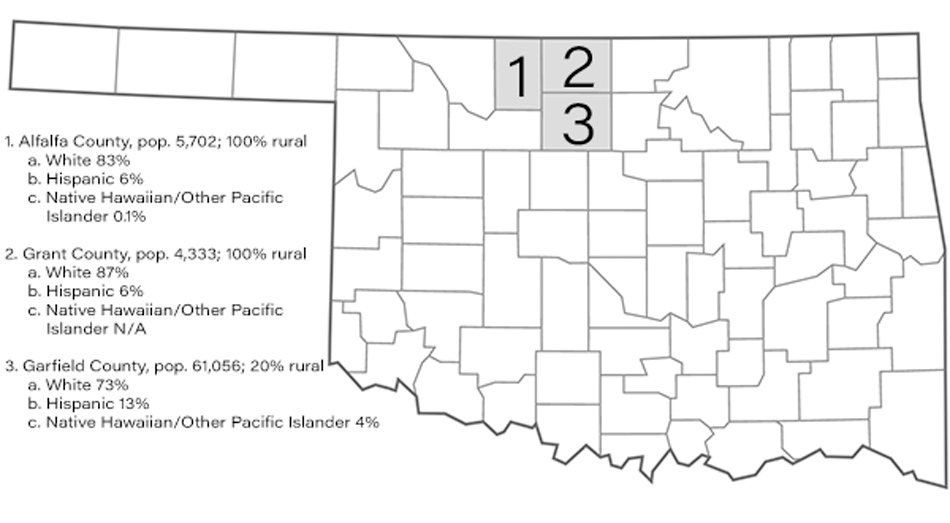
Tri-CHIO is a network that includes several local clinics and hospitals and serves — as its name implies — the rural population of three counties located in north central Oklahoma: Alfalfa, Grant, and Garfield counties. Leading up to the recent RHND award, previous HRSA funding support allowed Tri-CHIO to complete a Community Health Needs Assessment (CHNA), implement the Community Diabetes Education Outreach Program, and train a CHW.
Seigars shared that, with the 2017-2020 RHND funds, Tri-CHIO wanted to expand CHW work and hire additional staff to network with local primary care practices in order to implement best practices for chronic disease self-management. A third goal was to provide community resource coordination for patients with special needs identified by the primary care clinicians and emergency room providers.
CHWs and Community-Based Nonprofit Organizations

Seigars said that using CHWs for outreach to both the Hispanic and Marshallese communities within the three-county area has proved an effective method of offering several evidence-based programs: the Chronic Disease Self-Management Outreach Program (CDMOP), the Diabetes Empowerment Education Program (DEEPTM), and Prevent Type 2 Diabetes. Nearly 350 individuals from all of the area's ethnoracial groups participated in these educational offerings.
Though CHW work is effective, Seigars also shared that CHW recruitment and retention is a challenge.
“In our region, we're unique in the way that we use our CHWs,” she said. “Because Tri-CHIO's CHWs are usually in a public setting delivering group public presentations on diabetes and chronic disease management as opposed to the office setting where most of the region's CHWs are employed, recruitment is a challenge. Not every CHW is comfortable in that very public and group setting.”
Because there is no reimbursement mechanism for their CHW work, Seigars said that sustainable CHW employment is dependent on grants and other financial awards, sometimes making it difficult to guarantee ongoing employment for the organization's CHWs. Despite these challenges, she said she is very proud of the work their CHWs have accomplished in engaging the tri-county area's population, especially members of the Hispanic and Marshallese communities.
Culturally Competent CHW Outreach
The fact that Tri-CHIO demonstrated success of CHWs within the Hispanic community comes as no surprise, since the effectiveness of that specific CHW outreach is well-documented. For example, another previous FORHP-funded grantee in Arizona serves as an often-cited model.
What is unique about this Oklahoma effort is the trailblazing CHW work within the Marshallese community with the program, HOME or Health Outreach to Marshallese in Enid. The HOME program offers culturally competent healthcare navigation services to the nearly 3,000 Marshallese people in the tri-county area.
A Brief History of Marshallese People
According to a January 2021 report from the Centers for Disease Control and Prevention (CDC), Marshallese people “are from the Republic of the Marshall Islands (RMI), a chain of 5 volcanic islands and 29 coral atolls situated in the central Pacific Ocean halfway between Hawaii and Australia.”
From 1946 to 1958, RMI was the site of a nuclear weapons testing program that impacted food sources and the RMI population's overall health. The U.S. military continues a presence in the RMI and the Marshallese people have “the right to visit, reside, work, and study in the United States without a visa.” They pay taxes and serve in the U.S. military at greater per capita rates than U.S. citizens, according to the CDC report.
After welfare reform legislation in 1996, their eligibility for government-supported public services like health insurance was eliminated. However, the recent December 2020 Consolidated Appropriations Act (CARES) legislation has restored Medicaid eligibility.
In addition to the Oklahoma Marshallese community in the Enid area, another 12,000 live about 200 miles east in Springdale, Arkansas.
Seigars said Marshallese people are a very familial
culture and frequently travel back to their home islands
as well as to visit other U.S. Marshallese populations,
including the community in Springdale, Arkansas, about a
four-hour drive from Enid. In Enid, they've have had a
presence since 1970, primarily the result of missionary
work by faculty associated with a local university. Despite the
university's closure in 1998, the Enid population has
continued to grow, ranking as the fifth largest
Marshallese community in the U.S., according to Seigars.
Marshallese Population Numbers
Multiple professional sectors have expressed concern about the undercounting of the Marshallese population. A 2012 Census Bureau report indicated that the U.S.-based Marshallese population had doubled in size between 2000 and 2010, reaching over 22,000. Referencing the 2013-2017 American Community Survey results, a June 2020 Government Accounting Office report estimated the Marshallese population at over 25,000. Another academic report noted the population growth in the last decade actually might bring current numbers to 30,000, with the growth potentially related to physical changes occurring in the home islands.
Public health experts highlight the importance of
ensuring healthcare access for Marshallese people due to
the rates of non-communicable and communicable health
conditions experienced by the population.
Diabetes occurs at a rate 400% greater than in the
general U.S. population. In addition, they experience
disproportionate rates of communicable infections,
such as hepatitis B, tuberculosis, and Hansen's disease
(leprosy). It's important to note that, specifically for
the Enid Marshallese population, typhoid fever emerged as
a public health concern in 2015 when the Oklahoma
community experienced the
largest U.S. outbreak of typhoid fever since 1989. As
has been the case for other minority communities,
COVID-19 has also disproportionately impacted this
population, with the 2021 CDC report indicating that in a
two-county area in Arkansas, Marshallese people accounted
for 38% of the reported deaths during a four-month period
in 2020.
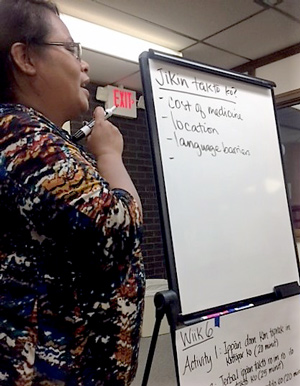
These facts highlight the importance of reaching Enid's Marshallese population. Seigars shared that previous efforts to engage the community were difficult for several reasons. For example, lacking insurance, many weren't able to access healthcare. When they did, they met language barriers and experienced cultural misunderstandings that made follow-up less likely.
According to Seigars, the key to engaging Enid's Marshallese community in the RHND grant's health education activities has been the efforts of Joelynn Karben, a Tri-CHIO CHW who was previously hired with monies associated with a private foundation's grant. In addition to her CHW certification, Karben worked as a CNA (certified nursing assistant) and is a member of the Marshallese community. With support from the current grant, Karben was able to provide cultural insights for the area's clinical providers in addition to providing the evidence-based chronic disease management trainings and navigation services for her community members.

For the latter community work, Seigars shared how Tri-CHIO leadership witnessed firsthand the power of using CHWs from the communities themselves: previous health education sessions had seen zero attendance, whereas “when Joelynn began providing the education, her community immediately began to attend, and attendance continues to grow.”
“After we hired Joelynn, people started showing up,” Seigars said. “When you can provide somebody who speaks the same language, who is from that community, and is a trusted source, people actually attend and are able to learn things that help improve their health.”
Karben provided additional information about her community and her work.
“In the Marshall Islands, for five dollars, we are able to go to the doctor any time, so that influences the way we keep appointment times,” Karben said. “It's also very important for us that women see female healthcare providers and men see male providers. Using our native language, Marshallese, during healthcare visits is very important to us. We are also a culture not used to the need for follow-up visits with providers.”
Seigars indicated that the local healthcare community has been able to accommodate the gender-based exam need, but that the language barrier has been more difficult to overcome. Karben said that she continues to emphasize the need for follow-up for chronic diseases, especially for diabetes since the rate is so high in the Marshallese population.
Karben said she often sees the impact of the education programs. For example, there is now increased clarity around the link between weight and diabetes. Classroom instruction on carbohydrate counting and how to read nutrition labels has allowed her community to enjoy their traditional foods as long as they remain mindful of carbs and sugar content.
Academic Research and Marshallese Culture
In a recent report, researchers at the University of Arkansas for Medical Sciences provide culturally competent recommendations for completing and interpreting a family health history.
Karben also shared some of the more personal rewards of
working within her community.
“Prior to the job, I was scared to speak in front of people,” she said. “But now I see that many people are making big changes regarding their health because of what I'm able to teach them. That gives me confidence to keep doing this work. And I'm always encouraging our younger community members to go into healthcare. We need more Marshallese healthcare providers in our community.”
Additionally, Seigars said her organization is proud of Karben's work in translating the chronic disease management material into Marshallese. This material will be now be available to others using DEEP and CDMOP.

Additional Successes
Other success stories associated with Karben's work:
- Group instruction allowed one attendee to take the knowledge home to share with other family members.
- As a recipient of Karben's navigation, appointment reminders, and translation services at the community's free clinic, one patient decreased their hemoglobin A1C from 14 to 8, a pattern also noted for other participants.
- Instruction has led to spontaneous formation of several long-standing support-like groups. For example, two years after an original DEEP class, a group of women still meet to encourage one another in weight loss and healthy living.
Leveraging Grant Funds: Creating a Live Resource Directory
Seigars said that though much of the grant funds do go to salaries, Tri-CHIO also uses funding to purchase reusable educational materials. Funding was also used to support another organizational goal: providing resource coordination.
“We held a community resource networking summit,” she said. “It was like a 'live resource directory' where we gathered everyone we could find that contributed to the diverse clinical and nonclinical patient needs. We asked attendees to complete an information sheet about their services and then grouped them into areas such as transportation, food, social services, in addition to healthcare. They were asked to present the organization's work in five or 10 minutes. We also invited other healthcare professionals like the hospital discharge planners and care managers since they are often looking for these types of needed community services for patients. These events also gave us a platform where we could share our services. Attendance even benefited our Tri-CHIO CHWs, allowing them to become even more familiar with our community resources.”
Sustainability: What's in the Future
Seigars said there are several promising future Tri-CHIO projects that build on the accomplishments of the completed work supported by the RHND grant: for example, potential contracts with the local healthcare providers where CHWs would continue to teach CDMOP and DEEP to the community at large and to selected ethnoracial groups. In particular, the work within the Marshallese community will continue. Additionally, there is continued activity around a resource directory.
“We are currently working with a company that has a platform that would allow us to enter our community resource information into an online, updateable directory, creating a so-called 'directory on steroids',” she said. “There's a lot of functionality within the platform, such as the ability to sort by language and desired services. For example, if you need food services for a Marshallese patient, you could search with those specific requests. We're hoping this becomes a reality for not just the professional organizations within our community, but for the general public as well.”

With a perspective gained from many years as a physician practicing in rural and urban locations, Dr. Kay Miller Temple writes on a variety of rural health topics and programs for RHIhub's Rural Monitor and Models and Innovations. She has a master's degree in Journalism and Mass Communication. Full Biography
View all articles by Kay Miller Temple