Oct 20, 2021
Out of the Shadows: Reducing the Rural Impact of Epilepsy
 "It is ridiculously common,"
said American Academy of Neurology (AAN) education chair
Dr. Joseph Sirven.
"It is ridiculously common,"
said American Academy of Neurology (AAN) education chair
Dr. Joseph Sirven.
A neurologist who specializes in the care of patients who have seizures — better known as an epileptologist — Sirven was talking about epilepsy and its importance as a rural public health issue. Sirven elaborated on the commonness of the diagnosis.

"This condition has an incredibly high disease burden globally, here in the United States, and definitely in rural America," he said. "It's associated with every age group, especially younger and older adults. And here in the U.S.? Over a lifetime, one of every 26 individuals will develop epilepsy. Not to be overlooked is the fact that it's a condition with high stakes: You can lose your right to drive, to fly, and you're likely to deal with significant stigmatization."
Sirven shared that, despite the condition's commonness, epilepsy continues to have a low profile because of its association with so many other conditions.
"No one ever chats about epilepsy," he said. "Instead, they talk about the conditions that cause seizures, from its link in premature babies born too small for their age, to Alzheimer's Disease, to stroke, to brain cancers, to traumatic brain injury. Epilepsy just doesn't get the attention. It's hidden. It's in the shadows."
Another epileptologist summarized why epilepsy awareness is an important public health focus.
"It's really as concerning as this: If you have a brain, you can get epilepsy," Dr. Gena Ghearing, a University of Iowa (UI) epileptologist, said.

Adding further to Sirven's emphasis on the high-stakes consequences of epilepsy, Ghearing pointed out, in particular, just how impactful the loss of driving privileges are for rural people with epilepsy (RPWE).
"For example, an urban epilepsy patient often has access to a subway system or city bus transit, but our patients living on a farm or in a small rural town usually don't have access to public transportation," she said, adding that family and friends might not even be able to provide transportation. "Not being able to drive just further compounds the many additional challenges of daily living for our rural patients."
Language Matters
Sirven also pointed out the importance of the language used around epilepsy.
"People come to me and say they have a seizure disorder, but they don't have epilepsy," Sirven said. "Why? Because epilepsy is called out in driving. Epilepsy is a seizure disorder and a seizure disorder is epilepsy. People get lost thinking that they're in the clear when they're not because of the specific consequences of epilepsy relative to driving or occupational activities."
Seizures and Epilepsy Defined: The Language Around Both
What is a seizure?
Johns Hopkins experts note that a seizure is a
sudden "burst of uncontrolled electrical activity" that
fires between brain cells. This electrical storm goes
right to the places these brain cells control. For
example, muscles can become stiff and rigid, can
twitch, or just go limp, causing a sudden unexplained
fall. Other times, this uncontrolled electrical
activity causes behavior changes, such as staring,
lip-smacking, or not responding to words. Sometimes
seizure activity can result in feeling a numbness
somewhere on the body or hearing sounds, like a
buzzing. The Epilepsy Foundation has more information
about
seizure types.
What is epilepsy?
According to the AAN's educational site, Brain
and Life, when a person has had two or more
unprovoked seizures — unprovoked meaning not related to
specific causes such as stopping alcohol if alcohol use
disorder is a problem, or low blood sugar if
diabetic — they are considered to have epilepsy. To
diagnose epilepsy, providers take a careful history
specific to the abnormal activity believed to be
indicative of a possible seizure. Then they review an
electroencephalography (EEG), a test that measures the
brain's electrical activity, very similar to the way an
EKG records the heart's electrical activity. A third
test used to establish a diagnosis are X-ray scans that
look at the brain structure, like an MRI (magnetic
resonance imaging) or a CT (computed tomography).
What causes epilepsy?
Only one of every three people will have a clear
link of their epilepsy to a known condition. According
to the Epilepsy Foundation, common causes of
epilepsy by age are:
|
Newborns:
Infants and Children:
|
Children and Adults:
Seniors:
|
Epilepsy and Rural Population Health
Over and over again, experts reiterated that epilepsy is the hidden common disease. According to the Centers for Disease Control and Prevention (CDC), about 3.4 million people nationwide have epilepsy. Experts translated that national number further: if 60,000 people were in a football stadium, about 600 people might have epilepsy. Specific to rural Canadian and American populations, a 2018 systematic review analyzed epilepsy-related health outcomes. The researchers found one paper concluding that RPWE experienced worse health outcomes relative to urban-dwelling people with epilepsy, while the remaining five studies found no difference. However, the review's limitations led the researchers to suggest that there is a need for more research on epilepsy among rural populations.
With respect to public health interventions aimed at decreasing rural epilepsy cases and meeting the needs of RPWE, experts emphasized that efforts must start with understanding the condition's prevalence. In 2017, the CDC published the first report on state-level epilepsy case numbers among both adults and children. By state, prevalence ranged from an estimated 7,300 epilepsy cases in North Dakota to as many as 428,000 in California. Though experts said rural-specific data are somewhat scarce, two studies provide some information. A 2014 CDC-funded study looking at all-age samples in rural southeast Kansas used a unique approach and found that epilepsy prevalence was on the higher end of comparable national estimates, finding 17 cases per 1,000 population compared to about 10 cases per 1,000 population in urban areas. A 2015 paper examining epilepsy prevalence from birth through 18 years found that in low-income rural Kansas counties, prevalence was slightly lower than national estimates at five cases compared to six cases per 1,000 population.
Recent CDC-supported state-level work in South Carolina has provided other important insights around issues for RPWE in that state that, compared to urban epilepsy patients, RPWE with the condition have an:
- Increased frequency of medical comorbidities, such as asthma, cardiovascular disease, diabetes, and Alzheimer's Disease
- Increased frequency of neurodevelopmental comorbidities, such as cerebral palsy, intellectual disabilities such as fetal alcohol syndrome, Down's syndrome, and genetic disorders
"Yes, You Can Die from Epilepsy."
Experts also said it's important for those caring for RPWE to be aware of another important public health focus: epilepsy deaths. According to epileptologists, it's rarely recognized that people with epilepsy can actually die of epilepsy. Some of these deaths are attributed to SUDEP, or sudden unexpected death in epilepsy.
SUDEP crosscuts all ages. As the name suggests, it is an unexpected death that comes to 3,000 epilepsy patients yearly. The agency maintains a surveillance registry, primarily focused on the pediatric age group, though some states track these events in those up to age 20. Though no rurality data are available for this diagnosis, overall it is one of the leading epilepsy-related causes of death for those with the condition. SUDEP researchers also noted that despite advances in treatment, overall mortality rates in epilepsy are rising. SUDEP risk factors include uncontrolled or frequent seizures, such as generalized tonic seizures, seizures that begin at a young age, and missed doses of medicine. Experts emphasized the importance of not missing any doses of epilepsy medications and noted how this might be more challenging for rural populations who have decreased access to providers and pharmacies.
Epilepsy-related costs are another public health concern. Again, though no rural-specific data are included, a 2020 study looking at healthcare spending over 30 years found that in 2016, epilepsy accounted for $8.6 billion in direct costs, of which over 60% was paid by public insurance.
Self-Management Programs: Importance for RPWE
Emphasizing the need for patients' self-awareness and knowledge about their epilepsy diagnosis, a 2007 survey revealed "one sobering finding": 44% of responding Midwest neurologists noted that epilepsy patients themselves lack understanding about their condition. Experts pointed to self-management programs (SMPs) as a valuable option to meet this need. Rosemarie Kobau serves as the CDC's National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP) Epilepsy Program's acting team lead. She said her specific interest in the potential for SMPs for epilepsy started as she completed her graduate studies doing original research around epilepsy. She also shared why rural population health influenced her career's direction.

"As a first-generation immigrant living in an immigrant community, I have lived experiences with socioeconomic, cultural, healthcare access, and language barriers," she said. "My college years were spent in Newton County, Georgia, where I spent time with my friends and their families and on their farms. I fell in love with those rural communities and appreciated the amazing opportunity I had to witness rural life and culture firsthand."
Kobau reviewed how the agency has partnered with researchers, clinicians, advocacy groups, and patients in order to meet the needs of RPWE.
"As far back as 1975 when Congress commissioned the Plan for Nationwide Action on Epilepsy, the CDC has been involved with epilepsy," Kobau said. "We track co-occurring conditions and access to care through our research and surveillance system and also partner with epilepsy organizations like the Epilepsy Foundation to promote prevention, raise public awareness, and reduce epilepsy stigma."
With the agency's creation of the Prevention Research Centers Program (PRC), the needs of RPWE have been addressed by the work of a thematic research center in existence since 2007: the Managing Epilepsy Well Network (MEW). Kobau said this center has specifically tested epilepsy SMPs in rural areas.
"Most people think that epilepsy self-management involves only medication adherence," she said. "Though taking anti-seizure medicines as prescribed is fundamental to epilepsy self-management, many factors impact seizure frequency, such as insufficient or poor-quality sleep, stress, or depression. We know that patients benefit from learning how to adopt health-enhancing behaviors and from learning to track and avoid seizure triggers when possible. These types of learning activities are core to self-management programs."
Kobau pointed to several MEW programs proving effective for rural populations: HOBSCOTCH, with a focus on the epilepsy-related memory problems, tested in rural New England, and PACES, tested in rural areas of the Northwest, focusing on improving disease-related problem solving and self-efficacy, meaning the confidence and ability to control motivation and behavior.
She also pointed to a third program, referred to as SMART, that was developed by researchers at Case Western Reserve University. UI's epileptologist Ghearing is now co-leading the modification efforts of this program in order for it to better address the needs of rural populations. As a collaborative researcher with the MEW Network, Ghearing works at UI's Prevention Research Center for Micropolitan Community Health. She said her clinical experiences caring for epilepsy patients living in more remote settings give her an understanding that what works in urban can't always be scaled to rural. She emphasized the importance of transportation again and further linked it to rural broadband issues.
When rural people with epilepsy can't drive because of their condition, they're often faced with an additional challenge: no nearby epilepsy specialists and no way to get to one.
"When rural people with epilepsy can't drive because of their condition, they're often faced with an additional challenge: no nearby epilepsy specialists and no way to get to one," she said. "These transportation issues heighten the need for self-management programs, but we can't lose sight that for some rural patients, they're dealing with broadband limitations for both virtual appointments and online education."
Epilepsy Foundation: Addressing Education and Stigma

Sara Franklin is the Epilepsy Foundation's community engagement director. She talked about the organization's work with CDC to create Seizure First Aid training for schools, law enforcement, and other organizations. Over the past several years, Franklin said this training has met with marked success.
"There's a lot of myths around seizures," she said. "For example, inserting something into a seizing patient's mouth to prevent them from swallowing their tongue is the wrong thing to do. People need more education. In around 90 minutes, Seizure First Aid training provides the lay public with information about how to recognize different types of seizures, what to do when someone has a seizure, and when to call for emergency help."
As public health experts might predict, Franklin mentioned an additional valuable program result: decreasing epilepsy's stigma.
"We've also discovered from feedback that just providing education about epilepsy, the increased awareness about the condition decreases the stigma around the condition," she said, again noting that stigma is a major challenge for people living with epilepsy.

Seizure Safe Schools
Prior to the travel restrictions imposed by the COVID-19 public health emergency, Franklin shared that rural communities, in particular, have been receptive to the Seizure First Aid training. Additionally, she said these communities have been integral to the Epilepsy Foundation's nationwide initiative to pass Seizure Safe Schools legislation in all states. Franklin said core to this legislation is the seizure first aid training for all school personnel.
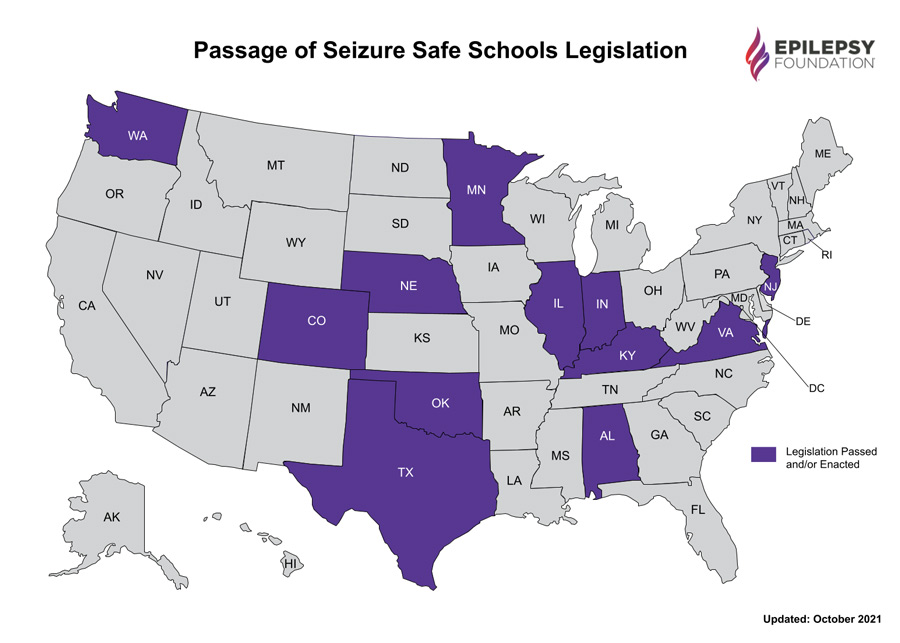
"For decades, medications to stop seizures could only be delivered rectally by a trained medical provider," she said. "That certainly caused barriers for a child in a rural school where a school nurse is not the usual. Now, these medications can be delivered nasally by people trained to do so. A child's life can possibly be saved if the nasal spray can be administered. Think what this means for a child. Think what this means for a parent. Think what this means for whoever is approved to deliver that medication."
Franklin said she is in absolute awe of the number of states that have enacted Seizure Safe Schools legislation: To date, 12 states have passed legislation, 3 more states have active bills, and for 2022 the foundation is advocating in 15 more states.
Educating the Rural Healthcare Workforce
Experts noted that for all chronic diseases, outcomes are time and time again linked to accessing knowledgeable healthcare providers. Getting clinical epilepsy information to rural providers is no exception. Though no rurality was included, a 2020 report looking at national survey data found that most participants with active epilepsy did see a general doctor. However, one in 10 patients did not see a general doctor or an epilepsy specialist within a 12-month period. This data point translates to 290,000 adults not accessing a medical provider.
This 2020 report supported findings from a previous study that included rural populations, the Connector's Project. Involved with the Connector's research, AAN's Sirven described details of its 2018 claims data analysis and mentioned several goals, including a better understanding of access to care for epilepsy patients in rural and other underserved areas.
"We learned there were two major barriers in moving the access needle: resources and having the right people and providers to connect to," he said, stating that the study also revealed other impactful upstream issues.
These studies and others with similar findings highlight the need to provide education for rural providers caring for RPWE. To meet this need, both Kobau and Franklin talked about their partnership supporting the University of Cincinnati's neurology/epilepsy Project ECHO®. Led by five university-based epileptologists, the group has also published participation outcome data. One participant who described their practice as located in "a very rural area" said, "It takes five months to get a referral to a neurologist and months for referral to psychiatry for patients with or without insurance…appreciate all insights related to what primary care can do."
 Epilepsy and the Community Health
Worker Curriculum
Epilepsy and the Community Health
Worker CurriculumUnderstanding the rural role of community health workers (CHWs) in addressing care gaps, Kobau pointed to CDC's new CHW training curriculum in epilepsy self-management. Used to train CHWs in Texas, New Hampshire, and other states, the formal training is provided by the HOBSCOTCH Institute, Dartmouth-Hitchcock Epilepsy Center.
Rural Epilepsy Clinical Care: Conversations from Healthcare Access to Driving
Stepping away from her research efforts, Ghearing spoke from her perspective as an epileptologist providing care to RPWE. She again pointed to the fact that because epilepsy is no less common in rural communities, RPWE need access to care in order to have a chance for good seizure control in order to live a quality life.
"If reimbursement is in alignment with providing epilepsy care, I do think we would do a lot more telehealth," she said. "We would be able to do similar with what we do for stroke. We could be involved with more first-time seizures, read EEGs remotely, offer quicker evaluation and diagnosis. Unlike the neurological diseases like Parkinson's Disease or multiple sclerosis that are usually dependent on a face-to-face neurologic exam, this is not usually necessary for epilepsy follow-up care."
She shared that only half of epilepsy patients are controlled with the first antiseizure medication they're prescribed, so follow-up care is really important for these RPWE.
"We have many of these medications and if one doesn't work, we have other options," she said. "What most people don't realize is that we have really effective treatment for refractory seizures. People with epilepsy in rural areas need to have equal access to this type of care."

Epileptologist Dr. Joseph Drazkowski said he also agrees that epilepsy telehealth outreach care for RPWE has much to offer. However, he added that one consideration surfaces: Some anti-epileptic drugs (AEDs) are controlled substances. This brings up similar barriers that have existed with rural medication-assisted treatment for opioid use disorder (OUD). The American Epilepsy Society's (AES) 2020 telehealth statement addressed these issues in the context of the COVID-19 public health emergency. Anecdotally, experts said some healthcare systems will not support their providers prescribing any controlled-substance AEDs in the virtual patient care setting.
As an expert in another high-impact aspect in the lives of RPWE, Drazkowski navigated from the medication prescribing restrictions to another restriction he said he believes is especially challenging in rural areas: driving.
"It's important to recognize that many medical conditions impact driving safety, but epilepsy is the condition called out by law," he said. "Every state in the country — and most countries in the world — have specific laws about driving with epilepsy. In essence, they brush aside other conditions that are equally as challenging."
Drazkowski's research and publications on epilepsy and driving has led to changes in state laws and exemptions of certain seizure types from driving restrictions. He said that although many crashes of all causes aren't reported, of those that are, only 0.4% are due to a seizure.
"It's also important to note that those seizure-related accidents that have caused serious harm or mortality are even below that, so actually it is generally very safe," he said, acknowledging that all accidents from any cause are tragedies that should be prevented by whatever means necessary.
Drazkowski said that inherent to living in rural America is travel over a larger geographic footprint than urban dwellers — and when that fact is combined with the common occurrence of seizures and an epilepsy diagnosis — Drazkowski noted that rural providers will have to have "the driving conversation" with their RPWE. He shared his approach: Recognize that the wrong approach might encourage under-reporting of seizure activity, know state law, educate regarding the consequences of driving should a seizure occur, and be optimistic.
Developing a relationship with the patient starts with being an advocate for the patient. Sometimes being an advocate means you can't drive. Sometimes it means you can drive.
"Developing a relationship with the patient starts with being an advocate for the patient," he said. "Sometimes being an advocate means you can't drive. Sometimes it means you can drive. Know the local law and the local exceptions. An example of one of those exceptions is the established pattern of seizures seen with nocturnal seizures."
He also said that with respect to driving, providers will need to be willing to do the "paperwork."
"I'll tell the patient we're going to answer any form's questions together," he said. "Sometimes they need to be coached a bit and given reminders that they don't want to hurt a grandchild, a neighbor, or their friends by driving. Most people have a sense of community and will respond to that."
He also emphasized the importance of optimism that is rooted both in good seizure control — and a look to autonomous driving technology.
"For patients, getting the best possible medical care means that about 70% of our patients will be able to drive because they're not seizing," he said, adding that he is very encouraged by what automated vehicles might bring to the lives of those who can't. He referenced a recent review of the technology, which he thought was especially important for rural areas, and said, "The technology's even there for curves, with uphill and downhill no longer a problem. I do believe this technology will crack the top-tier needs soon."
Drazkowski offered words of hope and optimism for those caring for RPWE.
"Try not to stigmatize epilepsy," he summarized. "Try to think of it as an illness like so many other chronic illnesses: It requires attention and it requires understanding. It requires up-to-date care. The days of phenytoin as the only available treatment drug are long gone. The days of multiple medications, alternative therapies, and device therapies are here. Down the road, there is only hope for the rural patient with epilepsy."

With a perspective gained from many years as a physician practicing in rural and urban locations, Dr. Kay Miller Temple wrote on a variety of rural health topics and programs for RHIhub's Rural Monitor. She has a master's degree in Journalism and Mass Communication.
View all articles by Kay Miller Temple