School-Based Health Center Dental Outreach
- Need: Improve the oral health of children age 3-17 in rural areas of Louisiana.
- Intervention: Leveraging 2012-2018 federal grant support, participating Federally Qualified Health Centers with school-based nurse practitioners were trained in oral health assessments and fluoride varnish application. When needed, dental referrals were also made. Interventions were tracked by dental case managers.
- Results: After grant cycle completion, these oral health interventions are now fully integrated into routine school-based care health examinations with intervention data included in required annual reporting.
Evidence-level
Promising (About evidence-level criteria)Description
A 2011 Pew Center report reviewing children's dental health noted that 40% of Louisiana 3rd graders had untreated tooth decay, with the state receiving a "D" after analysis of 8 dental-specific policy indicators. Tooth decay was also noted to be "one of the greatest unmet treatment needs among children. Pain and suffering associated with untreated dental disease can lead to problems with eating, speaking, and learning,” according to a 2016 Morbidity and Mortality Weekly Report. By 2021, the U.S. Preventive Services Task Force recommendations included the "application of fluoride varnish to the primary teeth of all infants and children starting at the age of primary tooth eruption in primary care practices."

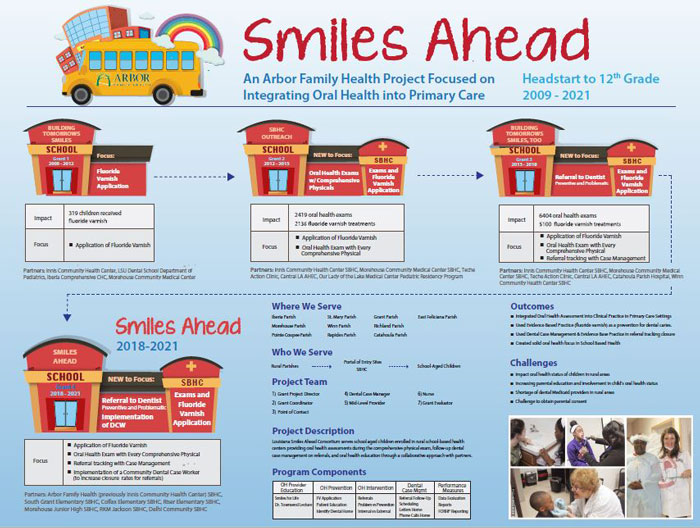
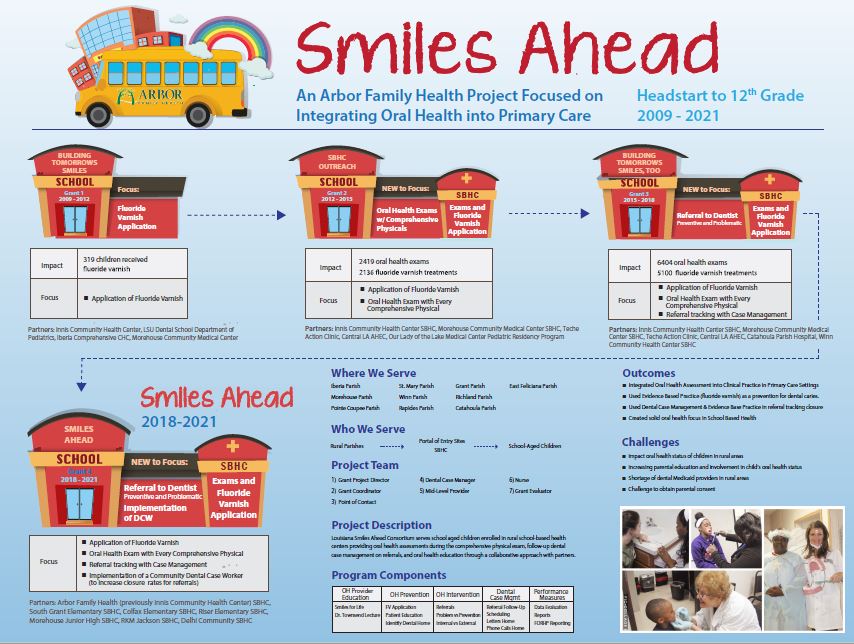
To meet the school-aged children's oral health needs in Pointe Coupee, Avoyelles, Iberville, Morehouse, Richland East Feliciana and Grant parishes, Louisiana's Arbor Family Health — formerly Innis Community Health Center, Inc. — integrated oral health into a primary care setting by leveraging federal funding through a 2012 and a 2015 Rural Health Care Services Outreach Grant awarded by the Federal Office of Rural Health Policy (FORHP).
Leading the effort, Arbor Family Health formed a network of four Federally Qualified Health Centers (FQHCs) to participate, with all sites creating a children's portal of access through existing school-based health centers (SBHCs) that were already delivering primary medical and behavioral care in their communities.
To provide the oral care, school-based advanced nurse practitioners received training to perform focused oral health assessments and interventions during comprehensive physicals. When indicated, they applied fluoride varnishes and referred children to dentist partners when other dental interventions were needed. This infrastructure and workflow facilitated integrating primary oral health care into routine primary medical care that also provided students with a dental home. Key to the work was collaborating with the area's dental providers, often a challenge with the area's dental provider shortage.
Although grant-support assistance helped sustain this care, early in the 2012 grant cycle, primary care providers' recognized many dental referrals were never completed. This discovery led to a 2015-2018 FORHP outreach grant award that supported a focus on dental case management. Case management, as described by the Case Management Society of America, provides care coordination that, specific to this need, helps navigate barriers to completing dental care appointments.
As of 2026, this approach to school-based oral healthcare is fully integrated into comprehensive school-based care, with oral health no longer separated from the rest of medical care. Age-appropriate oral health education is also integrated with medical health education. Because fluoride varnish is inexpensive, no outside funding is needed for its continued use. Case management continues. Additionally, when fluoride varnish application became part of the 2022 Core Set of Children's Health Care Quality Measures, grant participating FQHCs reported high percentages on this intervention.
Services offered
Sustained oral health activities linked to the original grant-funded work:
- Oral health training for providers working in the SBHC primary care settings.
- Oral health exams integrated within the comprehensive physical exam.
- Fluoride varnish application as an evidence-based preventive practice.
- School-based oral health education also integrated into age-appropriate health education, anticipating that this education can influence the oral health of subsequent generations.
- Dental case management.
- Electronic health record data tracking for oral health assessments, fluoride varnish applications, and treatment referrals.
- Internal tracking for FQHCs' Universal Data System (UDS) quality measures reporting with ongoing attention to ever increase even their current high percentages.
Results
Continued high percentage completion rates for integrated oral exams as part of a routine medical exam along with fluoride varnish application rates. Because of the previous grant focus, students, parents, and school faculty recognize oral health assessment as a normal part of a physical exam and is as critical as vision and hearing assessments due to oral health's impact on overall health and learning ability.
Previous grant cycle results:
2012-2015:
- SBHC providers were trained in oral health
assessments and fluoride varnish applications.
- Pre-2012-2015 grant assessment of SBHC capacity for oral health exams anticipated that 1,250, or nearly 41% of the target population would need fluoride varnish applications. Post-grant findings found that final applications exceeded that initial estimate by nearly 900, or 171% of the target goal.
- In addition to fluoride application, oral health caries risk assessments totaled 2,273, or 182% of the original target estimates. Despite these successes in identification of need, only 14% of those provided with a dental referral went on to complete that referral and establish a dental home. This result prompted the decision to initiate dental case management, implemented with the support of the 2015-2018 grant.
2015-2018 Outreach Grant Cycle results:
- 100% of providers became trained in oral health
assessments/fluoride varnish application through the
American Academy of Pediatrics program Protecting All
Children's Teeth.
- At grant cycle completion, data
tracking revealed:
- 6403 completed oral health assessments
- 5100 applications of fluoride varnish
- 2350 dental referrals averaged a 64% completion rate, substantially above the baseline 14% prior to dental case management implementation
With these grants' funding, dental case management emerged as key to the SBHC's oral health assessment program success, leading to an increased number of students ultimately seen by dental providers.
For more information on this program: The School-based Dental Center Dental Outreach is featured in the Oral Health Toolkit Program Clearinghouse.
- At grant cycle completion, data
tracking revealed:
Challenges
As with original grant work, engagement of dental colleagues continues as an intermittent challenge due to the low numbers of dental professionals in the area.
Replication
Because training primary care providers in basic oral health assessment and fluoride varnish application is achievable, the program is replicable in SBHCs and primary care facilities anywhere state laws allow the intervention. Referral follow-up is the key component that impacts the child's overall oral health status.
Some important strategies for success are:
- Oral health assessments integrated into the periodic comprehensive physical exam can generate revenue as a provider visit within the school-based health system
- Use electronic health record data-tracking for monitoring of follow-up
- Recognize that fluoride varnish is an inexpensive preventive evidence-based practice
- Sustainable SBHC dental case management can be sustainable when integrated with referral tracking on other referral types
Contact Information
Linda Matessino, RN, MPH, Grants Project DirectorArbor Family Health
225.921.5196
linda@arborfamilyhealth.org
Topics
Children and youth
· Delta Region
· Federally Qualified Health Centers
· Oral health
· Schools
· Wellness, health promotion, and disease prevention
States served
Louisiana
Date added
November 13, 2015
Suggested citation: Rural Health Information Hub, 2026. School-Based Health Center Dental Outreach [online]. Rural Health Information Hub. Available at: https://www.ruralhealthinfo.org/project-examples/861 [Accessed 7 August 2026]
Please contact the models and innovations contact directly for the most complete and current information about this program. Summaries of models and innovations are provided by RHIhub for your convenience. The programs described are not endorsed by RHIhub or by the Federal Office of Rural Health Policy. Each rural community should consider whether a particular project or approach is a good match for their community’s needs and capacity. While it is sometimes possible to adapt program components to match your resources, keep in mind that changes to the program design may impact results.